

“Tendonitis” Troubleshooting & Exercise “Quality” Profiles
“Tendonitis” Troubleshooting & Exercise “Quality” Profiles
Recovery Outlines for Tendinopathy Concerns - Progression Map and Details

“Tendonitis” Troubleshooting & Exercise “Quality” Profiles
Contents:
What is “Tendonitis”?
Factors to consider in management of pain and function
Common mistakes in rehabilitation and management
“What to do instead” - General outline of a pathway to recovery (Skip to here if you are lazy and like pictures)
Reverse engineering pain to get back to the demands of your performance
Rates of adaptation and expectations (Tendon remodeling rate vs inflection point of subjective symptom relief)
Fixing & Managing Tendinopathy

This post will cover some topics that have been covered in more detail in the previous “tendon properties” post - however for the sake of organization into something more comprehensive we will address some of the same information here. I do suggest that you read the last tendon post above in order to get the full picture if its necessary for you - but this post is meant to help guide you if you are suffering from a tendinopathy related problem and will be enough for those with mild cases.
If you want just the recovery outlines then just skip to that section way down there, but I highly suggest taking time to go through this whole post and others as the more informed you are the wiser you will be with your decision making when training yourself to recovery here as you are responsible for your own decisions with this information.
Note: None of this is medical advice, I am not a practicing physician. This is simply educational material based on my knowledge and personal practice. Consult a physician or your physical therapist if you are suffering from a health concern.
What is “Tendonitis”?
Tendonitis, or tendinitis, is a condition characterized by inflammation of a tendon. It often occurs due to overuse injuries, which are common in athletes who play their sport frequently or laborers who perform repetitive actions throughout the day.
However, it's worth noting that the term "tendonitis" is often used when it should really be referred to as "tendinopathy" because chronic conditions are the ones that are usually diagnosed. In most chronic issues, inflammation of the tendon is not actually the issue itself, as inflammation can be reduced, but the tendon damage still remains. Tendonitis itself without real pathological tendon damage is common and will heal in 2-4 days with nothing but bed rest in many cases. Chronic tendon degradation is a separate issue that involves actual structural issues deep in the tissue. Thus, most tendon issues that persist and cause concern for individuals are usually considered a case of tendinopathy and not tendonitis itself, even if tendon inflammation is present and a factor in management.
From this moment on, I will refer to the pathological issue that concerns populations with long term issues more generally as tendinopathy.
Though this may seem semantic - it matters because it helps you understand the difference in concern between issues which creates a different approach to recovery & management.
What Is Happening to my Joints?
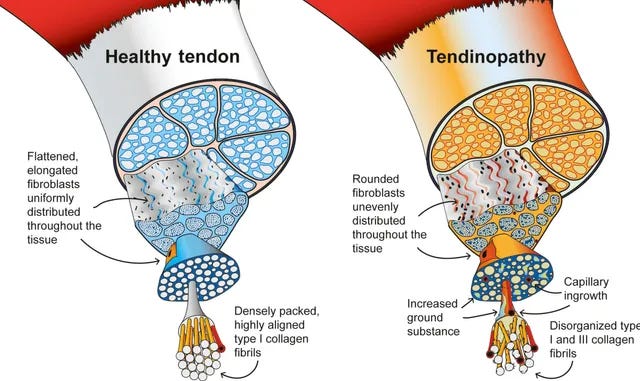
In pathological cases of tendon issues, it is usually due to a deformation of the tendon structure caused by repetitive trauma that did not resolve itself in the short term. This occurs when tendons are stressed through their primary functions, such as elastic storage and release (e.g. jumping or sprinting) or mechanical strain contribution (e.g. heavy lifting or repetitive strength efforts), leading to deformation of the tissue. Deformation is typically a breakdown of collagen fiber layers that make up a tendon and provides its strength (along with an intra-fiber gel that makes the tissue elastic at high speeds). This causes blood vessels to expand into the tendon territories, bringing more blood to them, and nerves to grow into the tissue to sensitize it to pain when detecting upticks in inflammation (tendonitis). Pain often eventually occurs due to the new "alarm system" that has been installed into the tendon structure.
Essentially - the inflammation that normally occurs in the body to promote healing and adaptation is now being responded to by the nervous system much more sensitively. You might picture this like when a division or employee at your workplace has a dysfunctional issue or episode and then a supervisor is sent down to observe them - common behavior is now more likely to be scrutinized and the workers are also much more encouraged to be on their “best behavior”.
In your case - your joint hurts when you do “X” and now, due to pain, you are hesitant to do “X” and HOPEFULLY this allows time for the tendon to heal…
Note: As we have mentioned on this blog regarding pain before - the purpose of this mechanism is to create some pain to encourage you to rest and recover from stress so the tendon has a chance to heal. However, its also been noted before and is worth mentioning that deformation and damage to a tendon does not mean you will necessarily by symptomatic, posses any painful response, or even be in danger of loss of function. Deformation and damage are simply risk factors for tendinopathic issues but not a guarantee. Many individuals have very deformed connective tissue under scans but perform perfectly fine - we are resilient animals.
Factors to consider in Tendinopathy Risk, Management of Pain and Function
Pain shows up AFTER the problem has been around a while
One of the more interesting notes is that the above process of blood vessel and nerve ingrowth begins to take place weeks prior to pain onset. It is typically the increase in stress (more training load, volume, or novel tasks) OR a loss of recovery ability (psychological stress, sleep, nutrition, etc.) that leads to an accumulation of damage to tendon structures that begin a process of building a pain response through nerve growth into the tendon. The nerves will then respond to inflammation levels that you previously were unresponsive to from a nociception (pain) standpoint.
Whatever pain you are experiencing now - it is the culmination of some behaviors or stressors from weeks prior. This will be important to understand later.
Deformation of a tendon is a RISK FACTOR for pain, but not a guarantee.
As mentioned prior, structural integrity of the tissue may incite a tendinopathic symptom response OR may impede function - or it may not. Many people have deformed tendons and it is not an issue and they function at virtually 100%.
However, it is a good idea to try and address damages and deformities to the structure in a tendon for the sake of prevention of future pain, as well as keeping a tendon healthy as we progress through life and new training phases.
Tendons have a low metabolic rate & access
Tendons are notorious for having “poor blood flow”. This is partly true but for accurately it is that tendons just generally absorb and interact with metabolic resources at a much slower rate even when in periods of higher contact. (Tendons that are “inflamed” actually have higher blood supply than usual).
However compared to tissues like skin and other rapidly regenerating organs/systems tendons just interact with the rest of the bodies nutrient supply less actively.
Note: This is a net positive adaptation that we possess. By being less dependent on blood supply the tendons that allow our musculo-skeletal system to function at baseline prevents us from losing total movement capacity if we go through any sort of low resource period, disease, etc. Muscle loss is more acceptable than tendon wasting as a smaller muscle is LESS strong but a smaller or missing tendon is catastrophic. Low blood flow means a tendon can work on its own with less nutritional dependence.
The downside to all of this is that when the tendon is “cooked” it can take MUCH longer to heal fully than other issues (much more important issues on this below)
Metabolic health greatly affects connective tissue quality
While tendons do have greater survivability under low nutrient and blood supply - it is STILL dependent on some nutrient and metabolic processes long term.
(See the previous tendon post on properties and tendon nutrition list here)
Its been observed that many factors can crush the recovery and collagen synthesis properties of a tendon related to metabolic health - completely unrelated to typical approaches of strength training & passive modalities like stretches and massage etc.
As elaborated on in the above linked post, tendons require various nutritional elements to repair and maintain themselves (even though their overall process is less active than muscle tissues). Despite being less responsive - they DO still operate as a reactive tissue and do need a supply of nutrients regardless of the tissues work rate.
Other factors like systemic inflammation due to chronic un-wellness & obesity, diabetes, dietary responses, lack of protein, other recovery factors like sleep and psych health etc can all deteriorate or diminish the bodies ability to promote the processes of proper healing when tendons need repair (which - like all body tissues - is daily).
Its been observed that diabetic patients in middle age have similar tendon tissue quality to other individuals between 90-100 years old. The rate at which they can handle and recover from stress is MUCH lower and essentially massively increases tendon rupture risk over time.
Vitamin C in particular is very important for collagen synthesis (which is the building of collagen tissue that makes up/repairs a tendon each day when you rest). Vit C deficiency reduces collagen tendon fiber repair up to 50% compared to those considered Vit C supplied. This is compounded further when more damage to a tendon occurs and thus the demand for extra collagen synthesis is even higher than usual.
Note: Its also been noted that collagen supplementation might not be relevant at all to the repair of a tendon for several reasons. However, this is not 100% clear and it is unlikely that you would not benefit from higher glycine and proline in your diet so collagen inclusion into your diet (through foods and possibly supplementation) is typically still a good idea.
Tendons have several functions in loading and movement

Though you should have read the tendon training series (5 parts linked above) to become familiar with this, we can summarize that tendons are largely made up of collagen links and a intracellular gel, both of which are essential to a tendons typical movement functions.
Collagen fibrils are used to be loaded up heavy and provide strength to the structure. They are used to absorb and pull muscle & bone upon high loading forces. They are very strong but still pliable so they can respond to both high loads and long muscle lengths.
The “intra-fascicular gel” that resides within the tissue provides a stiffening ability when the tendon is acted upon quickly. Under the higher impulse tensions from jumping, sprinting and catching your bodyweight - the gel provides a fast acting stiffness to the tissue so it can create propulsion.
The model I use to break up stress factors for both performance improvement but also injury management is length, load, and speed.
Tendon Shielding
A tendon is typically not completely damaged even when significant structural damage occurs. In almost every case, despite damage to part of the tendon, the tendon's function may still be at 100%, except for the pain response and perhaps muscle inhibition due to the perceived weakness. The cross-links of a tendon can redistribute force among healthy tissues and relieve compromised areas. This means that the protective mechanism referred to as tendon shielding can actually hinder your ability to stimulate and repair the damaged portion of the tissue in some cases.
Loading strategies will need to be specific to bypass this issue and actually stress the damaged fibers to realign, if this is occurring.
Tendons work WITH muscles and bones
Tendons function is to cooperate between a muscle and a bone as a piece of a “pulley” system and thus can only be functionally stressed by being pulled on with adequate tension. This means the tension and impulse that either a muscle OR bone applies to the tissue must be both adequately stimulating and not overly damaging in order to produce a favorable adaptation.
Tendons might be too strong relative to a muscles contractile strength for muscular efforts to be directly effective by actually challenging the tendon and bone to tendon contractions (plyometrics) can be dependent on the mechanical strength of a tendon if it is compromised enough and that can only be fixed through heavier loading.
Common mistakes in understanding, rehabilitation and management
Google any injury and you will receive and immediate recommendation of R.I.C.E. and NSAIDs. Even in 2023 this ancient piece of advice is medical information industry standard.
Horrible.
Read on.
This is covered in the previous tendon post as well but for the sake of making a more comprehensive single resource I am also mentioning these here. If you’ve already read the previous post - skip this section if you’d like and jump right into the recovery map.
R.I.C.E
Rest
We have covered this in the prior post with more depth but its worth reiterating that any rest period over 1-2 weeks is both beyond the point of usefulness and is actually quite harmful. In fact - after 2+ weeks of total bed rest (rare that one is totally immobilized but it happens with some populations) the muscle function can be aggressively diminished. In typical populations you will have noticeable decline in a few weeks of non-simulative training across several qualities.
This ruins the muscles ability to function as well as overall health/fitness (important as mentioned above) and when you do return to activity you are now even more compromised rather than recovered. This leads to several bigger problems when it comes to continuing with the rehab process.
The tendons are typically stronger than the muscle is - which both need to be stimulated enough to strain in order to adapt and get stronger. When muscle is already weaker than tendon and then diminishes its force capacity further you often cannot load a tendon heavy enough or with enough work to force it to adapt. Now you are forced to bring a muscle back up to former strength levels WHILE suffering from tendinopathy issues just to have a chance at beginning to actually create meaningful changes to the tendon later.
Don’t give yourself an extra step to overcome on an already potentially lengthy timeline of recovery. Begin training the area in some capacity you can tolerate within 1-2 weeks of recognizing the issue. In many cases you can continue training it the whole time while using methods to de-load the stress level lower temporarily with no full rest period or time off taking place at all.
On top of this total rest when a tendon is damaged enough will degrade its strength even further. Its ability to handle any mechanical load on the healthy parts of the tissue will diminish because they will simply “detrain” and become less conditioned to the stress of mechanical loading and store-release functions (lifting and running).
Thus you will compromise your ability to perform actions that you could have tolerated sooner had you not abandoned activity for so long.
Resting excessively past a 1-2 week period can turn a mild case of tendonitis pathological.
In this case you will take a situation where 1/4 of your life savings is in jeopardy and then you start blowing away the rest hoping the other quarter comes back later.
Ice & NSAIDs
Cold exposure can potentially be alleviating in some case in the acute and early phase of some injuries - however the case for alleviating natural inflammatory processes in order to treat an injury is obviously ass-backwards. Inflammation is part of the recovery process - its potential to cause discomfort is just a necessary side effect at times.
Reduction of the inflammatory process is short term gain for long term loss. Avoid icing and especially avoid the use of NSAIDs (They will destroy tendon health long term + a myriad of other complications in the body. Avoid unless absolutely necessary in the short term only).
Compression & Elevation
These are essentially irrelevant to anything in my opinion and we should all just leave it at that.
As a side note: Massage is often considered a form of passive “compression” therapy and it does absolutely nothing for a tendon or any connective tissue. Tendons are among the most durable “soft” tissues in the body and poking or massaging them will do nothing for their health.
The only indirect exception to this is that massage can help one relax and downregulate the nervous system effectively - this can actually be a good thing as it can help alleviate stress and temporarily numb you to symptom fixation and thus improve overall psychological status which can aid recovery in a indirect way.
So in this case - I am FOR massage or anything with no health costs if it makes you feel good. Feeling good = better health = better everything. But it does NOT “break up adhesions” or “stimulate healing tissues” etc.
Not loading or stressing the tissue enough
Typically many rehab protocols give you exercises > principles. People respond to this because they don’t want to do any thinking (understandable because you have 150 other problems to solve in life) so they ask for an exercise to “fix their knee”. Sometimes this works but sometimes it does not. This is often because it is not the exercise protocol given that will actually challenge your body’s capacity.
Often due to the fear of placing others in harms way, legal issues, or personal concern for individuals coaches & therapists will provide very low stress exercises to build the tissue capacity back up.
This may work when strength is very compromised but it also tends to “help” in the sense that it forces people to rest and deload their training protocols.
Half the benefit of little pink dumbbells and sticking to that (when it does slightly help) is just that the individual is forced to regress their stress loads on the tissue. Beyond that being useful it serves only to leave you spinning your wheels.
You need to progressively strengthen the area and seek to actively pursue greater capacity by stressing the body to get stronger - and not stagnate performing “3x10 wrist curls with 4lbs” for 5 months.
This takes an understanding both how to target the area with load and how to push that load further without taking too high of a jump between steps.
A favorite slogan I have adopted is being “aggressive with your rehab but smart with your progressions”.
Training only “Pain-Free”…
The reality is that flare ups in pain are not the exact same thing as degradation in capacity. Typically due to the nerve-pain response you are likely suffering from, normal inflammatory responses that typically would have been tolerated without major pain will simply feel more sensitive. Thus you may feel a tendinopathic pain response despite not necessarily having regressed or reinjured yourself in any serious way.
Pain is generally going to be a part of recovery - it is just about how much and when.
As a rule of thumb, if pain is subjectively exceeding 3 or 4/10 (meaning pain is beginning to be very difficult to ignore even if its not seriously intense) then you will want to tone total training/life stress down or address general health & recovery if that is compromised in the form of sleep or nutrition etc.
You need to develop tissue capacity by getting structurally stronger and develop a nervous system/psychological capacity by creating new experiences with using the joint that boost your confidence and heighten expectations of a pain free or more comfortable performance.
Expectations
Understand that if tendonitis (the mild inflammatory condition) is occurring - then it will simply dissipate after a few days to potentially a couple weeks if it is allowed to rest. However, true tendinopathic issues that become chronic and have broken into deeper fibers of the tendon will both regenerate OR be compensated for at a much slower manner than some like to expect when compared to other adaptations we seek in physicals training (i.e. muscle gain, fat loss, endurance improvements etc).
Often an approach will need to be looked at in the form of several months, and not days/weeks.
This leaves room for you to be pleasantly surprised if a recovery is ahead of schedule however, it prevents you from making a critical error in the process by understanding this.
If you get discouraged from the process 1-2 months in when it would be month 3-4 when symptomatic improvement would be noticeable then you will be more likely to divert from the plan and possibly fail when you were very close to a recovery.
A common experience is one gets hurt, takes a break, comes back and realizes they are still hurt, takes another break, comes back again with a worse issue and then tries “rehab”. They “attempt their rehab for 1-2 weeks at most before they fall off as symptoms didn’t improve. They might even feel slightly better during it and then attempt something they aren't ready for and reinjure. Often they will instead just fall into habits of avoiding what they once did in terms of fitness and leave themselves with the burden of a lingering constraint for an indefinite amount of time. These behavior cycles are the antithesis of what is required for success and thus it is crucial you are at least willing to be in this routine for several months without deviation.
Best case you are surprised by how fast you recover, worst case you are prepared for the journey.
Muscle and other tissue/function adaptations often are what improves symptoms and performance (not tendon repair)
It's important to note that tendon tissue healing is not always the sole cause of a successful rehab. Sometimes, it's the supercompensation of more muscle strength, movement adaptations, or other tissue and CNS changes that allow you to circumvent a tendon "hole" that may still exist. Either way, the result is virtually the same, and that is what we are chasing. The goal of rehab is not just to heal the tendon tissue, but also to improve overall function and performance. By focusing solely on the tendon tissue healing, we may miss out on the other adaptations that can lead to improved function and performance. Therefore, it's important to take a holistic approach to rehab and consider all aspects of the body and its function.
On top of this, as mentioned previously, muscle strength and its balanced cooperation with the tendon is a factor in injury as a muscle too weak to challenge a tendon that has been cooked is not going to allow you an easy pathway to actually stress and rehab the connective tissue. So training for more than “just the tendon hole” is valuable.
Progressions & Consistency
As mentioned earlier, inconsistencies in your habits are very common. If you struggle with knee tendon issues after playing basketball, and you play a lot, then stop playing altogether due to pain, and then jump back in again at the same volume once you "feel fine," you are likely to have the issue come back, perhaps worse, in a few weeks.
This can also happen during attempts at rehab. If you try rehab by finding some useful exercises, and then hammer them intensely for a session or two, but then take time off for other life activities, pain may flare up. If you realize you need to train and jump back in again, trying to make up for lost time, the issue may resurface.
Being consistent with your progression habits is more important than being intense with them in short periods. Due to various factors you may see symptom flare ups come and go during the process but there should be a general long term trend upward congruent with the steady climb in training stressors you place on yourself.
Fluctuations in volume and stress that are too high or frequent will be disastrous for many.
"What To Do Instead" - General Outline of a Pathway to Recovery
The theoretical outline for this strategy (which can be applied to any training goal, ultimately) is as follows: